

















 422 / 812
422 / 812

S418
24th European Congress of Psychiatry / European Psychiatry 33S (2016) S349–S805
EV214
First episode of bipolar depression
after systemic lupus erythematosus in
a 51-year-old woman
V. Tardelli
∗
, L. von Nielander , L. Sarin , J.A. Del Porto
Unifesp, Psychiatry, São Paulo, Brazil
∗
Corresponding author.
Introduction
Systemic lupus erythematosus (SLE) is a multi-
system disease with a broad spectrum of clinical features and
neuropsychiatric manifestations that occur in up to 60% of patients.
Disease activity and treatment with corticosteroids may contribute
to this higher risk. It is also known that 36% of patients with SLE and
comorbid Bipolar Disorder (BD) have had their psychiatric onset
after they had been diagnosed with SLE.
Method
Single case report.
Results
A 51-year-old woman received a diagnosis of SLE
24months before the beginning of depressive symptoms. After her
diagnosis of SLE, seven years ago, she had three suicide attempts,
being diagnosedwithmajor depressive disorder. Fromthemon, she
had crises characterized by well-defined periods of 7 to 10 days
with sadness, reduced need for sleep, social isolation, irritability,
anger outbursts, impulsivity, racing thoughts and suicidal ideation.
After treatment with mood stabilizers (quetiapine 300mg/day and
lithium 600mg/day), she had a substantial reduction of symptoms
intensity and frequency.
Conclusion
The link between immune dysregulation, autoimmu-
nity and bipolar disorder may be closer than previously thought.
Even if the autoimmune disease is not directly etiologically related
to the psychiatric presentation, its detection is important due to
the high morbidity and mortality, considering the current under-
standing that Bipolar Disease is strongly related with inflammation
in central nervous system.
Disclosure of interest
The authors have not supplied their decla-
ration of competing interest.
http://dx.doi.org/10.1016/j.eurpsy.2016.01.1199EV215
A major depression or a bipolar
disorder type 2? A cased-focussed
psycopathological and
psychophysiological challenge for a
resident
I. Targa
1 ,∗
, J. Soler
2, T. Gómez Alemany
31
Hospital Germanes Hospitalàries, Hospital de dia de Granollers,
Granollers, Spain
2
Hospital de dia, Hospital de dia, Granollers, Spain
3
Hospital de dia, Hospital de Granollers, Granollers, Spain
∗
Corresponding author.
A 41-year-old woman is diagnosed with a major depression after
a few weeks of having been operated of a stomach reduction
(bariatric surgery). She goes into old antidepressant medication for
a few weeks with an increasing worsening of her state, at the point
she is sent to the emergency room with high irritability, intense
agitation, suicide thoughts as the highlight symptoms of what we
think to be a mixed episode of a bipolar disorder and how we ori-
ent the case during hospitalization. The patient follows both public
and private psychiatric services and after discharge fromacute hos-
pitalization, still with residual depressions symptoms, her private
psychiatrist substitutes the given treatment, including mood sta-
bilizers, by only antidepressants. Two weeks after discharge from
the hospital, the patient is relocated to our partial hospitalization
resource. During her stay in our resource, we decide to keep the
new treatment and diagnosis and increase the dosage of one of the
antidepressants, which immediately yields to hypomania symp-
toms, at what we conclude that our patient is better treated as
a bipolar type II with a mood stabilizer and low doses of an SRI.
We find this to be an interesting case in the both psychopatho-
logical and psychophysiological point of view. To understand the
case beyond clinical diagnosis, we discuss profoundly whether the
bariatric surgery may have a role as a trigger.
Disclosure of interest
The authors have not supplied their decla-
ration of competing interest.
http://dx.doi.org/10.1016/j.eurpsy.2016.01.1200EV216
Descriptive study of patients with
bipolar disorder and dyslipidemia
E. Tercelan Alvarez
1 ,∗
, M.P. Sierra San Miguel
2,
L. Livianos Aldana
2, C. Gomis Martinez
1, V. Rodriguez Garcia
1,
C. Gómez González
1, L. Gonzalez Hernandez
1,
M. Anibarro Tienda
1, C. Ortigosa Silva
11
Hospital Universitario San Juan de Alicante, Psychiatry, San Juan de
Alicante, Spain
2
Hospital Universitario y Politècnico La Fe de Valencia, Psychiatry,
Valencia, Spain
∗
Corresponding author.
Introduction
It is known the relationship between mental dis-
orders such as bipolar disorder and metabolic disorders such as
dyslipidemia, and therefore, increasing comorbid pathologies such
as heart disease.
Objectives
Determine in patients diagnosedwith bipolar disorder
and dyslipidemia, which are the epidemiological characteristics,
the diagnostic subtype and drug treatment prevalent.
Aims
Determine the profile of patients with bipolar disorder and
dyslipidemia.
Methods
Creation of a database and conduction of a descriptive
study with statistical analysis of the data extracted from the med-
ical records of 100 patients from a public hospital.
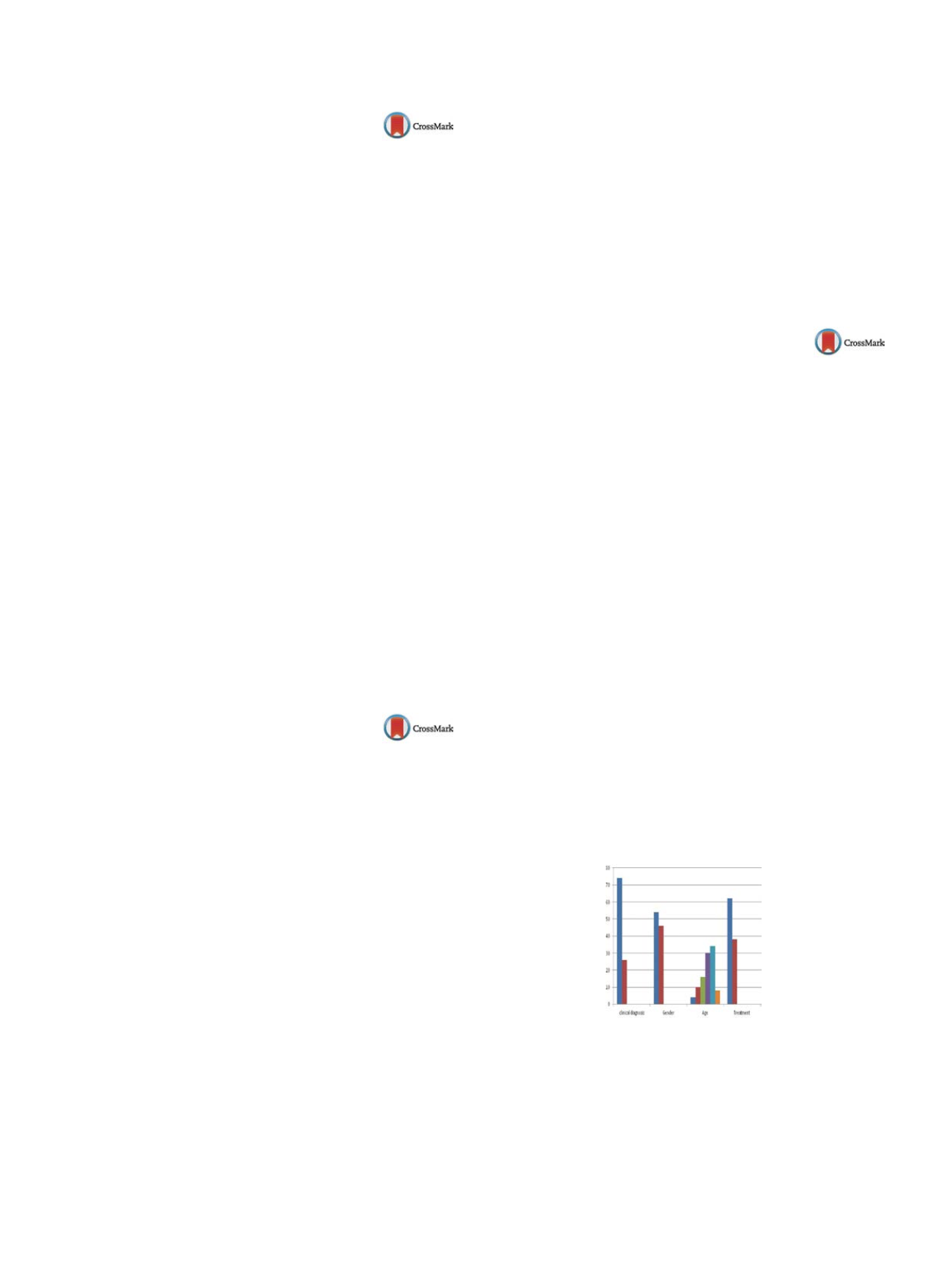
Results
Higher prevalence of diagnosis of bipolar disorder type I
on II (74% and 26%), male (54%) over female (46%), the age range
of 40–50 years, treated with antipsychotics more mood stabilizers
(62%) compared to mood stabilizer monotherapy (38%)
( Fig. 1 ).Conclusions
Interventions should be conducted screening char-
acter and in patients with a diagnosis of bipolar disorder type I,
male, age between 30–50 years, treated with mood stabilizers plus
antipsychotics (with a preference for lithiumassociationwith olan-
zapine).
Fig. 1
Disclosure of interest
The authors have not supplied their decla-
ration of competing interest.
http://dx.doi.org/10.1016/j.eurpsy.2016.01.1201